



|
The intervertebral discs are located between each vertebrae in the spinal column. Of the vertebrae, there are 7 cervical (neck), 12 thoracic (mid-back) and 5 lumbar (low back) discs. The discs make up approximately 1/3 of the spinal column. They have three main functions: (1) "Absorb shock" from everyday wear and tear. (2) Allow movement of our spinal column. (3) Separate the vertebrae.
The intervertebral disc is actually a type of cartilaginous joint. Discs consist of an outer layer, annulus fibrosis, and an inner nucleus pulposus, which is a soft, jelly-like, substance. The disc is made up of proteins called collagen and proteoglycans that attract water. Normally, discs compress when pressure is put on them and decompress when the pressure is relieved. These discs do not have a blood supply; therefore, they exchange nutrients by a process called "imbibition". Imagine a sponge filled with water; when that sponge is compressed, the water is forced out of the sponge. When the compressive force is removed, the water is "sucked" back into the sponge. This is precisely how discs stay healthy and functional. Diseased discs can lead to degenerative disc disease that can then lead to: arthritis, herniated discs, bulging discs, facet syndromes, sciatica and spinal stenosis
A herniation describes an abnormal condition of an intervertebral disc. Some refer to this condition as a "slipped", "ruptured", or "blown" disc. Most of the time it is not known what caused the disc to herniate, but it is thought to occur from repetitive stress due to occupation, poor spinal posture, and/or natural processes of aging and/or trauma.
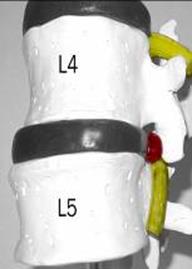
A herniation begins when the inner nucleus pulposus bulges through the annulus fibrosis, causing a bulging or protruding disc. This bulge may push on a spinal nerve. This interferes with the natural blood supply to the nerve roots and sets up a condition known as intraneural edema. Basically, the nerve root microcirculation is compressed and can progress to the point where the nucleus begins to leak out of the disc.
At this point the body begins to fight back by launching an autoimmune response to the disc material (nucleus pulposus). The reaction of this defense mechanism causes severe inflammation and progressive deterioration of the nerve root.
If the herniation is located in the cervical spine (neck), the symptoms can range from neck pain, with or without arm pain, to numbness and tingling. Muscle weakness can be common as well.
If the herniated disc is located in the lumbar spine (low back), the symptoms can range from low back pain, with or without leg pain, to numbness and tingling. Muscle weakness is also common.
This type of pain and/or numbness in the legs or arms is referred to as a "radiculopathy". This happens because the nerves that exit your spinal cord innervate ("attach to") the skin in your arms and legs. They are responsible for sensation and for movement of the muscles in your arms and legs. They are also responsible for the reflexive movements as well. This is the reason some individuals with these conditions experience extremity (leg/arm) pain / numbness / tingling and/or weakness when they have a herniated or bulging disc.
Be aware that, some individuals with herniated discs may report arm or leg pain only, with minimal neck or low back pain.
DIAGNOSIS
Diagnosis of a herniated disc (either neck or low back) can be made from a thorough physical examination including a detailed history, orthopedic and/or neurological evaluation.
Some disc patients will present with an antalgic gait (lean away from the side of the disc lesion), extremity pain/numbness/tingling (abnormal sensation) in addition to neck or low back pain. Muscle weakness may be present in the more chronic cases as well as areflexia ("loss of reflex").
X-rays can be helpful in identifying degenerative changes of the vertebra, but MRI’s are the "gold standard" to identify the exact nature of the lesion. When the disc is herniated in the lumbar spine (low back), and it is compressing the spinal nerve roots causing pain and numbness down the buttocks, thigh and leg, it is often referred to as sciatica.
TRADITIONAL TREATMENTS
Traditional treatments for herniated disc includes physical/chiropractic therapy, epidural Injections, surgery and pain killers such as non-steroid anti-inflammatory medication (NSAID's).
Please keep in mind that NSAID's have an inherent risk of gastrointestinal (GI) ("stomach" and "intestinal") disorders such as: perforation, ulceration and hemorrhages. The New England Journal of Medicine reported that it has been conservatively estimated that 16,500 NSAID-related deaths occur every year in the United States, and conservative calculations estimate that approximately 107,000 Americans are hospitalized every year due to NSAID related GI complications.
The number of deaths reported in the same study due to AIDS was 16,685. In addition to gastrointestinal disorders, drugs such as VIOXX have been known to cause serious cardiovascular (CV) events such as: heart attacks, strokes and heart failure. There have been similar complaints from other NSAID's such as: Bextra and Celebrex.
NON-SURGICAL SPINAL DECOMPRESSION
Non-Surgical Spinal Decompression offers to treat the root cause of the diseased or pathological disc based on the anatomical and physiological principles of Non-Surgical Spinal Decompression.
Non-Surgical Spinal Decompression relieves pressure from the disc, which, in turn, relieves pressure from the nerve.
According to the FDA 510k papers, the definition of decompression is “unloading due to distraction and positioning”, and additionally, “unweighting due to distraction and positioning”. This is important because the “unloading” of the injured area creates positive changes in the microcirculation of the disc and nerve roots.
Non-Surgical Spinal Decompression for herniated discs can have the following effects. Decompression of the involved disc which then takes pressure off the involved nerve root Reduction or elimination of extremity (leg/arm) pain and/or numbness, The pumping motions, due to Non-Surgical Spinal Decompression, called, "imbibition", allows nutrients to be exchanged at the level of the disc and inflammation around the nerve root to be dispersed resulting in reduction or elimination of low back pain.
LEG PAIN/SCIATICA This pain is most commonly experienced at the outside of the thigh, the lower leg and/or the foot. Shooting pain that radiates down the leg is a common experience with herniated discs. Patients commonly report an electric shock type of symptom.
PARASTHESIAS This is the medical word for abnormal sensations such as tingling, numbness, weakness or “pins and needles”. These symptoms may be the result of a herniated disc and may be experienced in the same regions as painful sensations.
BOWEL OR BLADDER PROBLEMS These symptoms are important because they may be a sign of Cauda Equina syndrome. This condition is possibly caused by a herniated disc. This is a medical emergency! You must see a medical doctor immediately if you have problems urinating, having bowel movements, or if you have numbness around your genitals. All of these symptoms are likely caused by irritation to one of the nerves as a result from a herniated disc.
MUSCLE WEAKNESS Signals from the brain may be interrupted due to nerve irritation. This can cause muscle weakness, usually of the ankle. Nerve irritation can be tested by examining the reflexes of the knee and ankle. EPIDURAL INJECTIONEpidural injections ("injection within the epidural space of the spinal cord") with corticosteroids, lidocaine or opioids have no proven benefit in treating neck or upper back symptoms.
In the instances that people find improvement, the effects are often temporary and require repeat injections, and several per year are not uncommon.
There is also an increase in risk in contracting a spinal infection that can lead to meningitis. In fact, the results of a randomized, double-blind trial, published in the June 2003 issue of the Annals of Rheumatic Diseases indicated that an epidural steroid injection was no better than an epidural saline ("salt water") Injection (i.e. placebo) for sciatica. These findings are consistent with those of another definitive trial presented at the last American College of Rheumatology meeting.
Given that there have been advances in spinal surgery, the outcomes can still be very unpredictable. In failed back surgery, post-operative pain syndrome is a very disabling and troubling reality of surgical intervention. According to the 2002 Johns Hopkins White Paper on “Low Back Pain and Osteoporosis “* by John P. Kostulk, M.D. and Simeon Margolis, M.D., PhD., surgery "is not the treatment of choice for most people with back pain." The report goes on to say “fewer than 5% of people with back pain are good candidates for surgery”. "Surgery ought to be used when all other measures have been explored, and only if it appears that there is a strong probability that it will improve the condition."
An article in Spine reviewed the outcomes and complication rates for surgical intervention in degenerative disc disease. Complication rates were as high as 55% and included: hematoma, neurologic adjacent segment degeneration, infection and hardware/instrument-related issues.
Another study determined the effects of single-level (2 vertebrae) and 2-level (3-4 vertebrae) spinal fusion success rates reported 53% with "good" and "fair" results with single- level fusion and no "good" results with 2-level fusions.
Having read about the possible side effects relating to these “traditional” treatments, you might want to consider the drugless, non-surgical approach that Non-Surgical Spinal Decompression has to offer.
· Wolfe, Michael MD et al. Gastrointestinal Toxicity of Non-Steroidal Anti-inflammatory Drugs. N Engl J Med. 1999 June 17; 340(24): 1888-1899. · Singh, G. Recent considerations in nonsteroidal anti-inflammatory drug gastropathy. Am J Med. 1998 Jul 27; 105(1B):31S-38S. · Soloman SD, McMurray JJ et. all. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med. 2005 Mar 17;352(17): 1071-80.Kostulk, John P. M.D., Margolis, Simeon M.D., PhD Johns HopkinsWhite Paper on Low Back Pain and Osteoporosis 2002. · Glass, Lee MD. Occupational Medicine Practice Guidelines: American College of Occupational & Environmental Medicine. 2nd ed., OEM press. · Bono, Christopher MD, Lee, Casey MD. The Influence of Subdiagnosis on Radiographic and Clinical Outcomes After Lumbar Fusion for Degenerative Disc Disorders: An Analysis of the Literature From Two Decades. Spine. 30(2):227-234, 2005. · Knox BD, Chapman TM. Anterior Lumbar Interbody Fusion for Discogram Concordant Pain. J Spinal Disord 1993;6:242-244.
|
|
Disk herniation’s |
|
Failed Back Surgery Syndrome Relieved by Chiropractic Click to View Video |
|
MRI Scans Show Immediate Benefits of Chiropractic Click to View Video |